Abstract
Background: Physical restraint can be defined as any act that avoids a person's liberated body change to a position of preference and, or regular evaluation to their body by the application of any technique, attached or adjacent to a person’s body that they cannot manage or remove easily. Inappropriate use of physical restraints may cause patients grave damage. Different studies informed that patients faced to physical restraints pass on due to pneumonia, constipation, and incontinence, as well as circulatory and respiratory problems. Critical care nurses should make correct decisions regarding use of physical restraints if they are to guarantee patient safety by the accountable nurse. Aim: the intention of this study was to assess nurses’ knowledge, attitude and practice; towards physical restraints use. Method: study design was a descriptive cross Sectional that used to assess knowledge, attitude and practice of nurses towards physical restraints in Orotta national referral hospital with self-administered questionnaire. Lastly data was analyzed using SPSS version 26. Results: the study was conducted among 100 nurses. 60% of the respondents were females and the median age of the study participants was 28 (IQR=6) years, with a minimum age of 21 and maximum age of 50yrs. Most of the study participants 31% had age of 25 or less years. Majority of them were diploma level and did not take any physical restraint related training 55% and 84% respectively. Except in recovery (12%) and adult ICU (27%) areas, the number of nurses in medical, surgical and adult was similar (each 20%). More than ninety percent (94%) of the study participants were not aware of the presence of guidelines regarding physical restraint in their work area. Conclusion: In this current study we concluded that, there was no correlation between knowledge and attitude and also between attitude and practice. But there was correlation between knowledge and practice. Those who have good knowledge can practice well. Nursing implication: By evaluating the current nurses’ knowledge, attitude and practice, this study will contribute recommendation on the frequent training of nurses on physical restraints and possible avoidance of it or safe practice.
|
Published in
|
World Journal of Medical Case Reports (Volume 5, Issue 1)
|
|
DOI
|
10.11648/j.wjmcr.20240501.11
|
|
Page(s)
|
1-12 |
|
Creative Commons
|

This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited.
|
|
Copyright
|
Copyright © The Author(s), 2024. Published by Science Publishing Group
|
Keywords
Attitude, Knowledge, Nurses, Physical Restrain, Practice
1. Introduction
Physical restraint is defined as any action or process that avoid a person's free body movement to a position of choice and, or usual access to their body by the use of any method, attached or adjacent to a person's body that they cannot manage or take away easily
| [1] | Bleijlevens, M. H. C., Wagner, L. M., Capezuti, E., & Hamers, J. P. H. (2016). Physical restraints: Consensus of a research definition using a modified Delphi technique. Journal of the American Geriatrics Society, 64(11), 2307–2310. https://doi.org/10.1111/jgs.14435 |
[1]
. It can also be defined as, Physical restraining is the use of physical, chemical or mechanical tools and devices which allow the restriction of a part of a demented, agitated or confused patient's body to control/restrain the patient's physical movements to prevent the patient from harming and injuring himself, and to ensure safe treatment of the patient
| [2] | Çelik S, Kavrazlı S., Demiran E, Güven N, Durmuş O, Duran ES. (2012). Knowledge, Attitudes And Practices Of Intensive Care Nurses Related To Using Physical Restraints. Acibadem University Journal of Health Sciences 3(3): 176-183. |
| [3] | Demir A. (2007). The use of physical restraints on children: Practices and attitudes of paediatric nurses in Turkey. International Nursing Review 54(4): 367–374. |
| [4] | Eşer İ, HakverdiogluG. (2006). Deciding On Using A Physical Restraint. C. Ü. Journal of Nursing School 10(1): 37-42. |
| [5] | Kaya H, Aştı T, Acaroglu R, ErolS, SavcıC. (2008). Nurses’ Knowledge, Attitudes And Practices Related To Using Physical Restraints. Maltepe University Journal of Nursing Science and Art1 (2): 21-29. |
| [6] | Orhan MF, Yakut Hİ. (2012). [Knowledge, Attitudes And Practices of Pediatric Intensive Care Nurses Related To Using Physical Restraints] Türkiye Çocuk Hast. Derg. Turkish J. Pediatr. Dis. 6(3): 155-160. |
[2-6]
. The Joint Commission on Accreditation of Hospital Organization (JCAHO) “Provision of Care, Treatment, and Services standard” defines restraints in two categories: (1) physical, or “any method of physically restricting a person’s freedom of movement, physical activity or normal access to his or her body” and (2) chemical, or “inappropriate use of a sedating psychotropic drug to manage of control behavior
| [7] | Regan Judy J, Wilhoite Kerri, Faheen Uzma, Wright Arvis. The use of restraint in psychiatric settings. The Journal mental health series. Tenn Med. 2006Mar: 41-2. |
[7].
Physical Restraint is any manual method, physical or mechanical device, or equipment that immobilizes or reduces the ability of the person to move hi/her arms, legs, body, or head freely including waist, vest, wrist or leg restraints, hand mitts, chairs with table tops, full side rails, ‘net beds’ or ‘enclosed beds’, elbow splints, or tucking a patient’s sheets so tightly that the patient cannot move
Improper use of physical restraints on patients may cause morbidity and mortality risks associated with new onset or increased agitation or confusion, delirium, pressure ulcers, urinary incontinence, constipation, fecal impaction, bruising, skin tears, or changes in skin integrity, pneumonia, and nerve injury
.
Furthermore, other studies indicated that patients who have been subjected to physical restraints experience mental and behavioral problems such as fear, panic, anger, and rage, in addition to the changes in their blood chemistry
| [1] | Bleijlevens, M. H. C., Wagner, L. M., Capezuti, E., & Hamers, J. P. H. (2016). Physical restraints: Consensus of a research definition using a modified Delphi technique. Journal of the American Geriatrics Society, 64(11), 2307–2310. https://doi.org/10.1111/jgs.14435 |
| [9] | Berzlanovich, A. M., Schöpfer, J., & Keil, W. (2012) Deaths due to physical restraint. Dtsch ArzteblInt. 109: 27-32. |
| [10] | Hakverdioglu, G., Demir, A., & Ulusoy, F. (2006) Evaluation of emergency nurses’ knowledge on physical restraints. Türkiye Klinikleri J. MedSci. 26, 634-641 (in Turkish). |
[1, 9, 10]
. Coming to the influencing factor towards the use of physical restraint clinical decision- making is vital. Clinical decision making is a method of significant and discriminative thinking patterns with unreliable weight that nurses have to look when making decision about patient care and prejudiced by diverse factors, such as clinical experience, education, interpersonal connection, specially, age, gender and environment
. On the other hand studies stressed, clinical experience is a dominant feature in the clinical decision-making procedure
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
| [13] | Abeer El-Said, H. E. & Ragaa Gasim, A. M. (2018). Assessment of nurse's knowledge, attitudes, and practice regarding physical restraints among critical ill patients. National Journal of Advanced; 4(1): 15-22. |
[12, 13]
.
Therefore; PR is practiced frequently everywhere in the acute settings of the Orotta national referral hospital despite the side effects. Although the researchers didn’t find similar published studies in Eritrea, however from the researchers’ informal observation there is a delay in prioritization, how to use and when to use physical restraint and whether to use or to use other alternatives, and thinking about patient right increased risk of patients from restrain on time in concerning to these verity of their conditions which may affect the patient safety and quality of care. Most of the time nurses restrained patients without hospital guidelines or protocols and usually they do not consider patient right. Although there are different opinions on the acceptability of physical restraints, but both chemical and physical restraints are often used in intensive care units and the most prevalent is the PR. So, the improper or unusual use of PR causes several complications in the patient’s life, both physically and psychologically. Use of physical restraints is directly linked to nurses’ knowledge and attitude. So, it is essential to assess nurses’ knowledge, attitude and practice towards physical restraints in health care settings. However, there are no formal studies of knowledge, attitudes and practices of nurses towards physical restraints in health care setting in Eritrea. Therefore; the purpose of this study is to assess the current knowledge, attitude and practice of nurses’ on use of physical restraints. Finally after identifying the gap of the nurses’ KAP on PR, it can be helpful to pass necessary recommendations to alleviate or proper use of PR to the policy makers.
2. Methodology
2.1. Study Design
This study was a descriptive cross-sectional study design with a quantitative approach to assess nurses’ knowledge, attitudes, and practices of nursing staff at ONRH regarding physical restraints use.
2.2. Study Area
The study was conducted in ONRH and teaching hospital, at different wards and Emergency, ICU and recovery units. The hospital is one of the Eritrea’s tertiary hospitals that give health care services to the referred and self-referred patients from almost all the country. ONRH is the only hospital that has ICU and highly equipped emergency department in Eritrea. In addition to this, it has operating room with different s specialty and a recovery room that gives care to the post-operative patients. There are also different wards like medical and surgical reserved for adult patients with different cases. The hospital is located in Asmara, the capital city of Eritrea.
2.3. Study Population
All Nurses in Orotta national referral hospital (emergency, ICU, recovery, medical and surgical wards) that was actively engaged in patient care. During the data collection time a total of 100 nurses were working in the specific wards and departments of the hospital.
2.4. Sampling Method
The sample of the study was all nurses who had participated inpatient care in different wards. That means a complete enumeration or census method was used. The study included all nurses who had actively worked in patient care during the study period and excluded nurses who were not present during the study period, not willing to participate and those who were not actively participate in patient care.
2.5. Data Collection Tools and Methods
Data was collected using an open ended, self-administered questionnaire. That was adopted from a study done in Ethiopia
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
| [18] | Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50. https://doi.org/10.3390/geriatrics4030050 |
[12, 18]
and modified in our context. As all the study participants can understand English no need of translating the questionnaire into national languages. Data was collected from January to March by three BSc. in Emergency and Critical Care Nursing staffs. The questionnaire had four parts; that included:
Part I
Socio-demographic questionnaire was used to gather demographic information from nurses.
Part II
Prepared knowledge questionnaire was used to gather the nurses' knowledge associated to physical restraint, with multiple choice answers. Every question has three options (yes, No, I don’t know) with only one correct response.
Part III
Prepared attitude questionnaire was used to gather the nurses' attitude associated to physical restraint. In this section a three level likert scale, (agree, not decided, disagree) was used with only single right answer.
Part IV
A prearranged practice questionnaire was used to gather the nurses' practice linked to physical restraint, which comprises of multiple option answers. Every question had three choices (Always, sometimes, never) with only one right answer.
2.6. Scoring System for the KAP Questionnaires
This scoring system is adopted from a study done in Menofia University
| [20] | Om-Mohamed Abed El-Latief Nurses’ Knowledge, Attitude and Practice towards Safety Physical Restraint Zagazig Nursing Journal January; 2015 Vol. 11, No. 1. |
[20]
. Part1: nurses` knowledge regarding physical restraints.
This part includes ten items with ten correct answers and scored as follows: 1 = yes and 0 = I do not know or no.
1) The maximum score is 10 (1*10) (respondents remained positive (i.e., yes) to the positive statements)
2) Poor level of knowledge: it represents 0–5 (less than 50%)
3) A fair level of expertise: it represents 6–7 (from 50 to 75%)
4) Good level of knowledge: it represents 8–10 (more than 75%)
Part2: nurses` attitude regarding physical restraints among critical-care patients.
There are 11 items which include nine correct questions and two false questions scored by three-point Likert scale. Different responses were scored as follows: 2 = strongly agree/agree, 1 = non decided and 0 = strongly disagree/disagree.
1) The maximum score is 22 (2*11) (respondents remained positive (i.e., agreed) to the positive statements), and the minimum score is 0 (0*11) (respondents in this category remained negative (i.e., disagree)
2) Proper Attitude: it represents 14–22 (more than 60%)
3) Improper attitude: it represents 0–13 (less than 60%)
Part3: nurses` practice regarding physical restraints among critical-care patients.
There are 13 items, which includes ten correct questions and, one false question and two MCQs.
1) Different responses were scored as follows: 2 = Always, 1 = sometimes, and 0 =never
2) The maximum score is 22 (2*11) (respondents remained positive (i.e., always) to the positive statements), and the minimum score is 0 (0*11) (respondents inthis category remained negative (i.e., never)
3) Unsatisfactory practice; it represented 0–11 (less than 50%)
4) Satisfactory practice: it represented 12–16 (from 50 to 75%)
5) Good practice: it represented 17–22 (more than 75%)
2.7. Validity
The questionnaire was assessed its validity in the previous study and was found to have acceptable content validity index (0.90, 0.70, and 0.90 for knowledge, attitude, and practice respectively)
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
| [18] | Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50. https://doi.org/10.3390/geriatrics4030050 |
[12, 18]
. In addition, the validity of the three tools were assessed by a panel discussion of three experts from emergency and critical care nursing as a jury to test the study tools for content validity, completeness, feasibility and clarity of the items. Accordingly, all the necessary modifications were made.
2.8. Reliability
Reliability was measured to evaluate whether all items in the study instruments measure the same variable, and how all the used items fit together conceptually. The internal consistency of the knowledge (α=0.83) and attitude (0.70) scales were found to have acceptable reliability in previous studies
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
| [18] | Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50. https://doi.org/10.3390/geriatrics4030050 |
[12, 18]
.
2.9. Plan of Data Processing and Statistical Analysis
Data was coded, edited, entered, cleaned for discrepancies, and analyzed using SPSS, Version 26 software. Frequency (proportion) was used to explain categorical variables, while mean (SD), and median (IQR) was used to sum up the continuous ones, as appropriate. After verification of normality, independent variables were assessed using T-test and ANOVA to determine factors that affect knowledge, attitude and practice on PR. Variables that were significant at bivariate level using one way ANOVA further assessed using Least Significant Difference (LSD) method or the pair wise post-hoc comparisons. The association between the knowledge, attitude, and practice percentages was computed with Pearson’s correlation coefficient. P-values less than 0.05 were considered as significant association.
3. Results
3.1. Socio-DemographicVariables
The socio-demographic characteristics of the study participants are displayed in
Table 1. The median age of the nurses was 28 (IQR=6) with a minimum of 21 and maximum of 50 years. 60% of the participants were females with four or more years of experience (61%). More than half (55%) of the study participants were diploma in nursing. Most nurses did not take any physical restraint- related training (84%) and were duty nurses (93%). Except in recovery (12%) and a adult ICU (27%) areas, the number of nurses in medical, surgical and adult was similar (each nearer to 20%). More than nine type recent (94%) of nurses were not sure on the presence of guidelines in their work area regarding physical restraint.
Table 1. Socio-demographic variables of the study participants.
Variable | Frequency | Percentage |
Age (Md=28.00, IQR=6, Min.=21, Max.=50) |
| 25orless | 31 | 31 |
| 26to28 | 20 | 20 |
| 29to31 | 26 | 26 |
| 32ormore | 23 | 23 |
Sex | | | |
| Male | 40 | 40 |
| Female | 60 | 60 |
Work experience, years | |
| One | 3 | 3 |
| Two | 8 | 8 |
| Three | 28 | 28 |
| Four or more | 61 | 61 |
Level of education | |
| Certificate | 37 | 37 |
| Diploma | 55 | 55 |
| Degree | 6 | 6 |
| Masters | 2 | 2 |
Any related training | |
| Yes | 16 | 16 |
| No | 84 | 84 |
Current nursing position | |
| Duty nurse | 93 | 93 |
| Head nurse | 7 | 7 |
Work area | | |
| Medical | 20 | 20 |
| Surgical | 21 | 21 |
| Recovery | 12 | 12 |
| Adult ICU | 27 | 27 |
| Adult ER | 20 | 20 |
Presence of guideline in the work area |
| Yes | 6 | 6 |
| No | 94 | 94 |
3.2. Item-Wise Analysis of Knowledge of Nurses on Physical Restraint
About three-fourth of the study participants (73%) correctly knew that, physical restraint is simply acceptable to keep patients or other people from damage. More than sixty percent (64%) were correctly answered that, there might be risk of choking if a patient restrained though lying flat in bed. On the other hand, 26% of the respondents correctly knew whether there is inadequate time that a patient is able to restrain in your unit. The Majority of the participants (94%) were not correctly responded to the item “when they think physical restraint should be released if the patient is awake.”Other summary results of knowledge assessing items are displayed in
Table 2.
Table 2. Percentage distribution of study participants’ on physical restraint item-wise analysis (n=100).
Knowledge question | | Correct | Incorrect |
Do you know physical restraint is only allowed to prevent patients or other people from damage? | 73 | 27 |
Do you know there may be danger of choking if a patient restrained while lying flat in bed. | 64 | 36 |
When do you think physical restraint should be released if the patient is awake? | 6 | 94 |
Is there a limited time that an individual patient can be restrained in your unit? | 26 | 74 |
Nurses can be punished for threatening the patients if they use physical restraint when it is not required | 50 | 50 |
Records of usage should be kept for each patient who is restrained in every shift | 57 | 43 |
Only in emergencies, nurses are allowed to use the physical restraint on patients without any doctor’s instruction | 36 | 64 |
What kind of restraint do you know? | | | |
| Sedation | 72 | 28 |
| Massaging | 16 | 84 |
| Family involvement | 47 | 53 |
| Frequent monitoring | 40 | 60 |
Good reasons for use of physical restraint | | | |
| Confusion | 65 | 35 |
| Disorientation | 45 | 55 |
| Restless | 65 | 35 |
| Shortage of sedation | 34 | 66 |
3.3. Attitude Towards Physical Restraint Item-Wise Analysis
Table 3 shows the percentage distribution of nurses regarding their attitude towards physical restraint for each item. More than sixty percent of the nurses agreed/strongly agreed that family members have the right to reject the utilization of physical restraints (67%) and self-refusal on being restrained, if they were patients (63%). Almost three out of four of the participants also agreed/strongly agreed that physical restraint must be approved by a person in charge (75%) and feeling discomfort when they place a patient on restraint (73%). One out of five (42%) of the nurses agreed/strongly agreed that they sense uncomfortable whilst family members come in to the restrained patient’s room if they have not been informed. The remaining items and their results are displayed in
Table 3.
Table 3. Item-wise distribution of study participant’ according to their attitude towards physical restraint.
Attitude question | Strongly agree/agree n (%) | Not decided n (%) | Strongly disagree/disagree n (%) |
Do you think that family members have the right to refuse the use of physical restraints? | 67 | 10 | 23 |
Do you think that a physical restraint should be prescribed by a responsible body? | 75 | 7 | 18 |
If you were a patient, do you think that you have the right to refuse being restrained? | 63 | 12 | 25 |
Do you feel discomfort when you placing a patient on restraint? | 73 | 6 | 21 |
Do you feel embarrassed when family members enter the restrained patient’s room if they have not been informed? | 42 | 21 | 37 |
The hospital is responsible to adhering to the laws on the use of restraints to ensure the safety of a patient. | 76 | 11 | 13 |
Do you feel uncomfortable if a patient becomes more upset after being restrained? | 71 | 12 | 17 |
Do you feel that placing a patient in restraints can decrease nursing care time? | 57 | 3 | 40 |
Patients suffer from feeling inferior when they are restrained. | 57 | 23 | 20 |
Do you think it is important to apply restraints to assure legal protection for your self and your centre? | 67 | 12 | 21 |
Do you believe that restraints increase the risk of strangulation? | 50 | 18 | 32 |
3.4. Practice of Nurses on Physical Restraint Item-Wise Analysis
More than three quarter (77%) of the participants were reported, they try little nursing process before bodily restraining the patient. More than eighty percent (82%) of the nurses also agreed/strongly agreed that prior to use physical restraint on patient, they come across why they should to do it. More than three quarter (77%) of the participants responding to patients’ call for help immediately. One out of three nurses (60%) was able to inspect restrained patients at least on a two-hour basis. Eighty percent of the nurses also reported that they examine the patients’ skin for redness or bruised while giving personal care. Other practice-related results are displayed in
Table 4.
Table 4. Percentage distribution of study participants on practice of physical restrain.
Practice questions | Strongly agree/agree n (%) | Not decided n (%) | Strongly disagree/disagree (%) |
Do you try a few nursing methods before physically restrained the patient? | 77 | 12 | 11 |
Before using the physical restraint on the patient, do you find out why you need to do it? | 82 | 14 | 4 |
Did you respond to the patients’ call for help from a restrained patient immediately? | 77 | 7 | 16 |
Did you examine restrained patients at least on a two-hour basis? | 60 | 16 | 24 |
When giving personal care to the restrained patients, did you examine their skin to find parts, which are red or bruised? | 80 | 7 | 13 |
Did you tell the patients why they are restrained? | 62 | 15 | 23 |
Did you tell the family members/visitors why the patient is restrained? | 82 | 6 | 12 |
Did you restrain patients when you faced a staff shortage? | 26 | 17 | 57 |
Did you record the type of restraint, reason and the time on card? | 53 | 13 | 34 |
Did you assess the restrained patient frequently if the restraint should be removed? | 70 | 5 | 25 |
Did you evaluate and record the effect of physical restraint when applied to a patient? | 49 | 24 | 27 |
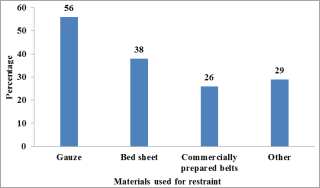
More than half (56%) of the study participants reported that gauze is used as a material for restraint. Followed to this, bed sheets (38%) and commercially prepared belts (26%) were used as a means of patient restraining. Other materials used for restraining were elastic bandage (25%), roll bandage (3%) and cotton and bandage (1%) as displayed in the
figure 1.
On the other hand, regarding the restrained patients’ body part wrist was (82%), followed by ankle (63%), chest (33%) and waist (23%) which displayed in
table 5.
Figure 1. Materials used for restraint by the nurses.
Other* includes mainly elastic bandage (n=25) and roll bandage (n=3).
Table 5. Part of the patient restrained by nurses.
Variable | Freq./% |
Part of the patient restrained |
| Wrist | 82 |
| Chest | 33 |
| Waist | 23 |
| Ankle | 63 |
3.5. Composite Knowledge, Attitude, and Practice Score
Composite scores of knowledge, attitude and practice were computed initially and then transformed to percentage. The total original score of knowledge, attitude, and practice assessing items were 15, 55 and 62. Then, the three total scores obtained from each study participant were transformed to percentage. After transforming the scores, normality was checked for each of them using measure of skewness (kurtosis). The measures for knowledge, attitude, and practice were 0.27 (-0.89), -0.59 (0.44), and 0.23 (-0.27). Since they were in the range of -1 to 1, they were treated as normally distributed.
Summarized results of the composite knowledge, attitude, and practice scores are displayed in
Table 6. The mean (SD) knowledge score was 48.27 (17.65) out of 100, slightly less than half. The minimum and maximum knowledge scores were 20 and 86.67. On the other hand, the mean (SD) attitude score was 62.22 (6.45) with minimum and maximum scores of 43.64 and 74.55 respectively. The mean (SD) practice score was 71.02 (11.34) with minimum and maximum scores of 45.16 and 100 respectively.
Table 6. Summary measures of the composite knowledge, attitude, and practice score.
Variable | M (SD) | Md (IQR) | Minimum | Maximum |
Knowledge | 48.27(17.65) | 46.67(26.67) | 20 | 86.67 |
Attitude | 62.22(6.45) | 61.82(9.09) | 43.64 | 74.55 |
Practice | 71.02(11.34) | 71.77(14.11) | 45.16 | 100 |
3.6. Factors Related to Knowledge, Attitude, and Practice on Physical Restraint
Factors that potentially affect knowledge, attitude, and practice were assessed using independent samples T-test and ANOVA across the different categories of the socio-demographic variables.
Table 7 shows composite score differences across different categories of demographic characteristics. Results revealed that the categories of age, sex, work experience, level of education, training related to PR, current nursing position, and awareness on presence of guideline did not have significant difference across knowledge scores. However, nurses who work at different work areas were found to have significant difference on knowledge score. Generally, nurses who work at medical and surgical wards were observed to have more knowledge scores.
Similarly, the categories of age, sex, work experience, level of education, current nursing position, and work area had similar attitude. However, nurses who had no training previously had significantly higher attitudes as compared to those nurses who had previous training (p=0.003). Nurses who were aware on presence of guidelines had also significantly lower attitudes towards physical restraint as compared to their counterparts.
The composite practice score was not significantly different across all the demographic variables investigated in the study.
Table 7. Composite score differences across different categories of demographic characteristics.
Variable | | Knowledge | Attitude | Practice |
| M (SD) | M (SD) | M (SD) |
Age | | | | |
| 25orless | 49.67(17.46) | 60.59(6.84) | 69.72(11.75) |
| 26to28 | 44.67(17.32) | 62.00(4.44) | 67.74(10.84) |
| 29to31 | 46.41(16.92) | 63.71(6.12) | 72.39(9.85) |
| 32ormore | 51.59(19.30) | 62.93(7.53) | 74.05(12.45) |
| F value | 0.705 | 1.232 | 1.384 |
| p-value | 0.551 | 0.303 | 0.252 |
Sex | | | | |
| Male | 47.17(16.22) | 61.50(7.55) | 72.30(12.92) |
| Female | 49.00(18.65) | 62.70(5.62) | 70.16(10.19) |
| t-value | -0.507 | -0.909 | 0.922 |
| p-value | 0.613 | 0.366 | 0.359 |
Work experience, years | | |
| Three or less | 47.52(18.87) | 60.65(6.65) | 69.15(11.52) |
| Four o rmore | 48.74(16.98) | 63.22(6.41) | 72.21(11.16) |
| t-value | -0.336 | -1.969 | -1.322 |
| p-value | 0.738 | 0.052 | 0.193 |
Level of education | | | |
| Certificate | 45.77(18.40) | 61.33(5.82) | 68.61(11.15) |
| Diploma | 48.85(17.78) | 62.94(6.59) | 71.88(10.99) |
| Degree/Masters | 55.83(11.23) | 61.36(8.35) | 76.21(13.52) |
| F-value | 1.139 | 0.767 | 1.858 |
| p-value | 0.324 | 0.467 | 0.161 |
Any related training | | | |
| Yes | 47.92(17.25) | 57.95(7.82) | 69.25(12.95) |
| No | 48.33(17.83) | 63.03(5.86) | 71.35(11.07) |
| t-value | -0.086 | -3.000 | -0.676 |
| p-value | 0.932 | 0.003 | 0.501 |
Current nursing position | | |
| Dutynurse | 47.67(17.47) | 62.29(6.27) | 70.83(11.22) |
| Headnurse | 56.19(19.57) | 61.30(9.01) | 73.50(13.59) |
| t-value | -1.235 | 0.390 | -0.599 |
| p-value | 0.22 | 0.698 | 0.550 |
Work area | | | |
| Medical | 56.00(15.05) | 61.00(7.79) | 68.63(12.64) |
| Surgical | 50.16(22.07) | 61.39(6.16) | 75.65(11.66) |
| Recovery | 39.44(15.16) | 63.94(3.18) | 66.53(12.55) |
| Adult ICU | 49.87(16.68) | 63.23(5.97) | 72.46(7.25) |
| Adult ER | 41.67(14.33) | 61.91(7.45) | 69.27(12.48) |
| F-value | 2.697 | 0.649 | 1.857 |
| p-value | 0.035 | 0.629 | 0.124 |
Existence of guideline in the work area | |
| Yes | 35.56(17.21) | 56.06(4.93) | 68.01(10.01) |
| No | 49.08(17.46) | 62.61(6.35) | 71.21(11.44) |
| t-value | -1.841 | -2.474 | -0.667 |
| p-value | 0.069 | 0.015 | 0.506 |
Post hoc comparison of knowledge score differences across the categories of the work area was performed after the significant ANOVA result was obtained. The result showed that nurses who work at medical ward had significantly higher knowledge score as compared to those who work in recovery (MD = 16.56, 95% CI: 4.18, 28.94). On the other hand, nurses who work at medical have significantly higher knowledge scores than those who work at adult ER (MD = 14.33, 95% CI:3. 61,25.06). The results are displayed in
Table 8.
Table 8. Post-hoc comparisons of the knowledge score differences across different work areas.
Comparisons | MD (95%CI) | p-value |
Medical Vs Recovery | 16.56 (4.18,28.94) | 0.009 |
Medical Vs Adult ER | 14.33 (3.61,25.06) | 0.009 |
3.7. Correlation among Knowledge, Attitude, and Practice
The composite scores of knowledge, attitude, and practice were assessed on their normality and then the correlation coefficient using Spear man’s correlation coefficient was computed. The result revealed no significant correlation between knowledge and attitude (r=-0.057, p=0.571) and attitude and practice (r=0.169, p=0.093). However, a significant correlation was observed between knowledge and practice (r=0.438, p<0.001). Hence, nurses who have more knowledge scores were observed to practice better.
Table 9 shows the matrix correlation of the potential relationships.
Table 9. Cross matrix correlation among knowledge, attitude, and practice toward physical restraint.
| Knowledge | Attitude | Practice |
Knowledge | 1 | -0.057(0.571) | 0.438(<0.001) |
Attitude | - | 1 | 0169(0.093) |
Practice | - | - | 1 |
4. Discussion
4.1. About Socio-Demographic Characteristics of Participants
The present study reported that majority of the participants (60%) were females, similar to this, a study carry out in South Africa concluded that majority of the participants (81.4%) were females
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
[12]
. Further studies, at Menoufia University, Egypt and Konya, Turkey, results reported that, most of their participants were females
| [14] | Kaya, H., & Dogu O. (2018). Intensive Care Unit Nurses’ Knowledge, Attitudes And Practices Related To Using Physical Restraints. International Journal of Caring Sciences, 11:1, 61-70. |
| [15] | Kandeel N. A. & Attia, A. K.: Physical restraints practice in adult intensive care units in Egypt. Nursing and Health Sciences. 2013; 15, 79–85. |
[14, 15]
. On the contrary the present study is different with the study done in Ethiopia, male and female distribution was almost equal (50.9%and49.1) respectively
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
[12]
. In the present study, regarding age, educational level, and year of experiences, most participants had age of 25 or less, diploma in nursing, and with professional experience of four or more. This result may indicate young nurses are employed in tertiary hospitals like Orotta than the bachelor’s as a policy. This is similar to a study done in Johannesburg, South Africa, Egypt, and Istanbul, Turkey
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
| [15] | Kandeel N. A. & Attia, A. K.: Physical restraints practice in adult intensive care units in Egypt. Nursing and Health Sciences. 2013; 15, 79–85. |
| [16] | Swee, G. L. and Vivian, J. T. (2021). Critical care nurses’ knowledge, attitudes and practices on the usage of physical restrainer. IEJSME; 15 (1): 5-18. |
[12, 15, 16]
; results showed that, ages between 21-30 years old and have a work experience of 2-5 years, but regarding educational level in those studies majority of the study participants were Bachelor’s which is in congruent to the current study.
In the current study 84% of participants were not sitting previously for training about physical restraints, and 94% reported that they did not have a guideline or a written policy for the utilization of physical restraint. This result indicates that most nurses were practiced without written guidelines and any training on the side-effect of PR. This study is congruent with survey conducted in Ethiopia
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
[12]
. Most of the study participants did not get any training before about physical restraints which are only about 29% of their study participants did receive training, and 69.6% responded that they did not have guideline or written policy for the use of physical restraint and, same is accurate with the studies done in Egypt, and South Africa
| [11] | Kalula, S. Z., & Petros, S. G. (2016) Use of physical restraint in hospital patients: A descriptive study in a tertiary hospital in South Africa. Curationis 39(1): 1-8. https://doi.org/10.4102/curationis.v39i1.1605 |
| [14] | Kaya, H., & Dogu O. (2018). Intensive Care Unit Nurses’ Knowledge, Attitudes And Practices Related To Using Physical Restraints. International Journal of Caring Sciences, 11:1, 61-70. |
[11, 14]
.
4.2. Nurses` Knowledge Toward Application of Physical Restraints.
In the current study almost 73% of participants correctly answered that physical restraint is simply allowed to safe guard patients or other people from damage, and 57% responded to records of practice should be kept for each patient who is restrained in each shift, in contrast studies conducted in Malaysia
| [17] | Fatma, B. & Fatmana, İ. (2019). The Knowledge, Attitudes and Practices of Nurses in Relation to the Use of Physical Restraints. International Journal of Health Sciences; 7(1): 18-25. URL: https://doi.org/10.15640/ijhs.v7n1a3 |
[17]
most of the critical care nurses, 96.1% recognized that physical restraint can be used to avoid damage and is only permitted to be used on patients for the purpose of safeguarding patients or others from injury and 96.1% study participants understood the magnitude of documenting the usage of physical restraint. In the current study 64% of nurses did not agree that physical restraint required doctor’s order and 50% of participants did not have information about official punishment. These results showed us most nurses practiced based on their previous knowledge and is not acceptable as it may cause legal consequences. This finding is congruent to the study made in Malaysia
| [18] | Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50. https://doi.org/10.3390/geriatrics4030050 |
[18]
, nurses were initiated and terminated the use of physical restraint based on their clinical judgment.
In this current study regarding the percentage of overall knowledge score, the study participants’ correct answer was 48%. This might be due to unavailability of written policy and guideline for use of physical restraint and, or the respondents didn’t get suitable training regarding application of physical restraint. This study supported by study conducted in Malaysia, and Ethiopia in different time periods
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
| [17] | Fatma, B. & Fatmana, İ. (2019). The Knowledge, Attitudes and Practices of Nurses in Relation to the Use of Physical Restraints. International Journal of Health Sciences; 7(1): 18-25. URL: https://doi.org/10.15640/ijhs.v7n1a3 |
| [18] | Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50. https://doi.org/10.3390/geriatrics4030050 |
[12, 17, 18]
. On the contrary survey conducted in Egypt revealed that, knowledge score was high than to the current study
| [14] | Kaya, H., & Dogu O. (2018). Intensive Care Unit Nurses’ Knowledge, Attitudes And Practices Related To Using Physical Restraints. International Journal of Caring Sciences, 11:1, 61-70. |
[14]
.
4.3. Attitude of Nurses Regarding Physical Restraint Use
In this current study, the most of the study participants, 63% agreed that patients have the right to refuse physical restraint, 67% of respondents agreed the patient’s family members can refuse restraint usage on the patient, and 42% agreed that the hospital is accountable to stick to the rule on practice of physical restraint. This finding implied that nurses are fully aware and attentive on patient’s right. Therefore, this will ensure that lawful and ethical implications can be avoided. The current result is more or less similar to a study conducted in Malaysia, 96.1%, 86.4%, and 98.1%
| [17] | Fatma, B. & Fatmana, İ. (2019). The Knowledge, Attitudes and Practices of Nurses in Relation to the Use of Physical Restraints. International Journal of Health Sciences; 7(1): 18-25. URL: https://doi.org/10.15640/ijhs.v7n1a3 |
[17]
.
In this current study, the correct attitude percentage response was 62.22%. This result is alike to a study conducted in Ethiopia (64%)
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
[12]
. But these results are higher than those reported in Egypt, Turkey and Malaysia
| [14] | Kaya, H., & Dogu O. (2018). Intensive Care Unit Nurses’ Knowledge, Attitudes And Practices Related To Using Physical Restraints. International Journal of Caring Sciences, 11:1, 61-70. |
| [15] | Kandeel N. A. & Attia, A. K.: Physical restraints practice in adult intensive care units in Egypt. Nursing and Health Sciences. 2013; 15, 79–85. |
| [18] | Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50. https://doi.org/10.3390/geriatrics4030050 |
[14, 15, 18]
.
4.4. Practice of Study Participants Regarding Physical Restraint
In the current study 77% of the study participants reported that, they tried few nursing methods before physically restraining the patient. 82% of the nurses also agreed/strongly agreed that prior to use the physical restraint on the patient, they find out why they need to do it before. And 77% of the study participants reported that, they respond to patients call for help immediately. Despite the nurses’ knowledge of physical restraint, in the current study nurse tries to support patient autonomy as well as to avoid harmful effect of physical restraint. These results are similar with the study conducted in Malaysia 72.8% responded positively on opting for options before applying physical restraint, in comparison, 88.3% specified that they would find out the motives on the need of physical restraint before deciding on applying it. 84.5% react right away to signal light or call for assistance from restrained patients
| [17] | Fatma, B. & Fatmana, İ. (2019). The Knowledge, Attitudes and Practices of Nurses in Relation to the Use of Physical Restraints. International Journal of Health Sciences; 7(1): 18-25. URL: https://doi.org/10.15640/ijhs.v7n1a3 |
[17]
. The present study also supported by a study conducted in London, England that was reported respondents’ judgment to minimize the use of restraints is determined by seem into the concrete grounds for using physical restraint, assessment of patients’ condition, and rectifying possible motive and hazards
| [19] | Mahmoud AS. Psychiatric Nurses’ Attitude and Practice toward Physical Restraint. Arch. Psychiatr. Nurs. 2017; 31: 2-7. |
[19]
. In contrast, other studies revealed that majority of the participants did not regularly inspect patient’s skin condition and speak well with patient
| [20] | Om-Mohamed Abed El-Latief Nurses’ Knowledge, Attitude and Practice towards Safety Physical Restraint Zagazig Nursing Journal January; 2015 Vol. 11, No. 1. |
[20]
.
The overall correct practice percentage was 71.02%, which coincides with the study done in Ethiopia, Egypt, and Malaysia
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
| [14] | Kaya, H., & Dogu O. (2018). Intensive Care Unit Nurses’ Knowledge, Attitudes And Practices Related To Using Physical Restraints. International Journal of Caring Sciences, 11:1, 61-70. |
| [18] | Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50. https://doi.org/10.3390/geriatrics4030050 |
[12, 14, 18]
, but slightly lower than the study done in Turkey
| [15] | Kandeel N. A. & Attia, A. K.: Physical restraints practice in adult intensive care units in Egypt. Nursing and Health Sciences. 2013; 15, 79–85. |
[15]
.
4.5. Factors Related to Knowledge, Attitude, and Practice on Physical Restraint
The present study revealed that, there was no statistical significance between study participants’ educational background and knowledge, attitude, and practice. This result is comparable with study made in Ethiopia and Egypt
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
| [13] | Abeer El-Said, H. E. & Ragaa Gasim, A. M. (2018). Assessment of nurse's knowledge, attitudes, and practice regarding physical restraints among critical ill patients. National Journal of Advanced; 4(1): 15-22. |
| [14] | Kaya, H., & Dogu O. (2018). Intensive Care Unit Nurses’ Knowledge, Attitudes And Practices Related To Using Physical Restraints. International Journal of Caring Sciences, 11:1, 61-70. |
[12-14]
. However, this study is different with the study done in Malaysia that demonstrated significant differences in knowledge scores between diploma and degree nurses, as nurses who had degree certification had higher knowledge scores than the lower levels
| [18] | Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50. https://doi.org/10.3390/geriatrics4030050 |
[18]
.
Regarding attitude related to previous training, the current study showed that, nurses who had no training previously had significantly higher attitude as compared to those nurses who had previous training. Nurses who were aware of the presence of guideline had also significantly lower attitude as compared to their counterparts. This difference may be either the training was taken before long time or they may not be fully attentive at the time of training. In Contrary, this result found to be different from the study done in Ethiopia and Malaysia, as the study participants who did not have previous training on PR had 2.6 times less knowledgeable than the trained
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
| [18] | Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50. https://doi.org/10.3390/geriatrics4030050 |
[12, 18]
. And this is also supported by the study done in Johannesburg, that policy and guidelines on the use of physical restraints, lead health practitioners in managing restrained patients
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
[12]
.
4.6. Correlation among Knowledge, Attitude, and Practice
In the current study results revealed that, there was no significant association between knowledge and attitude, and attitude and practice. Nevertheless, a significant correlation was observed between knowledge and practice. Hence, nurses who have more knowledge scores were observed to practice better. Unlike to the current research, study done in Ethiopia
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
[12]
showed there was significant correlation between knowledge and practice, which coincides with current study. Still, unlike to the current study, there was a significant correlation between attitude and practice
| [12] | Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa. |
| [13] | Abeer El-Said, H. E. & Ragaa Gasim, A. M. (2018). Assessment of nurse's knowledge, attitudes, and practice regarding physical restraints among critical ill patients. National Journal of Advanced; 4(1): 15-22. |
| [18] | Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50. https://doi.org/10.3390/geriatrics4030050 |
[12, 13, 18]
. Overall, this obscure those nurses’ practice levels enhanced with proper knowledge.
5. Conclusions and Nursing Implication
5.1. Conclusions
Physical restraint is an act putting patients with no access to their bodies. Although it widely practiced in acute settings but practicing without following written guidelines is not safe. So generally PR should not be use frequently except in certain times with the help of experts and under close supervision. In this study the results concluded that there was no correlation between knowledge and attitude, and also between attitude and practice. However, there was correlation between knowledge and practice. Those who have good knowledge can practice well. Based on these results we recommend that to do further research with large sample size and with interventional studies in order to improve the knowledge and practice of nurses so as to identify and prevent patient harms and to introduce better methods other than PR.
5.2. Nursing Implication
Knowledge, attitude, and practice of nurses towards nursing care is very important and its outcome is so fruitful. At the same time physical restraints in hospitals and other health care facilities is practiced prevalently. If this is practiced with poor KAP its harm on patients is high. So this study tries to identify and evaluate what done on the ground. Finally this will find the gap and recommend planning in-service training to all nurses for the better patient outcome.
Abbreviations
ER | Emergency Room |
ECCN | Emergency and Critical Care |
FDA | Food and Drug Administration |
HNRH | Halibet National Referral Hospital |
ICU | Intensive Care Unit |
IQR | Inter Quartile Range |
KAP | Knowledge, Attitude and, Practice |
ONRH | Orotta National Referral Hospital |
OCMHS | Orotta College of Medicine and Health Science |
PR | Physical Restraint |
WHO | World Health Organization |
Acknowledgments
We say thanks to the Research and ethical committee of the Ministry of Health and the OCMHS, the department of Nursing for excellent cooperation on this research. Also, we would like to thank all the nurses who participated in the study. Special thanks go to all others who made a significant contribution to this research.
Ethical Approval and Consent to Participate
The researchers obtain permission from the ethical committee of Orotta College of Medicine and Health Sciences, and Ministry of Health Eritrea at the department of research and human resource development. To be approved in the hospital and on the nurses. Then further permission was obtained from the study sites before carrying out the survey. Verbal and written informed consent was also obtained from the participants before conducting the survey.
Consent for Publication
The study does not enclose any entity details and consent for publication is not applicable.
Author Contributions
Hisabu Kidane: Conceptualization, Data curation, Supervision, Validation, Writing - original draft, Methodology, Project administration, Writing - review & editing
Merhawi Habtemariam: Conceptualization, Resources, Data curation, Investigation, Writing - original draft Methodology
Rahel Tewelde: Conceptualization, Data curation, Software, Formal Analysis, Writing - original draft, Methodology, Project administration, Writing - review & editing
Sulieman Mahmud: Conceptualization, Data curation, Software, Funding acquisition, Writing - original draft, Methodology, Project administration, Writing - review & editing
Eyasu Habte: Methodology, Writing - review & editing
Funding
This research was not received any grant from financial support agencies in the public, commercial, or not for profit sectors.
Data Availability Statement
Statistical facts and resources are available by the principal authors up on sensible request.
Conflicts of Interest
The authors declare no conflicts of interest.
References
| [1] |
Bleijlevens, M. H. C., Wagner, L. M., Capezuti, E., & Hamers, J. P. H. (2016). Physical restraints: Consensus of a research definition using a modified Delphi technique. Journal of the American Geriatrics Society, 64(11), 2307–2310.
https://doi.org/10.1111/jgs.14435
|
| [2] |
Çelik S, Kavrazlı S., Demiran E, Güven N, Durmuş O, Duran ES. (2012). Knowledge, Attitudes And Practices Of Intensive Care Nurses Related To Using Physical Restraints. Acibadem University Journal of Health Sciences 3(3): 176-183.
|
| [3] |
Demir A. (2007). The use of physical restraints on children: Practices and attitudes of paediatric nurses in Turkey. International Nursing Review 54(4): 367–374.
|
| [4] |
Eşer İ, HakverdiogluG. (2006). Deciding On Using A Physical Restraint. C. Ü. Journal of Nursing School 10(1): 37-42.
|
| [5] |
Kaya H, Aştı T, Acaroglu R, ErolS, SavcıC. (2008). Nurses’ Knowledge, Attitudes And Practices Related To Using Physical Restraints. Maltepe University Journal of Nursing Science and Art1 (2): 21-29.
|
| [6] |
Orhan MF, Yakut Hİ. (2012). [Knowledge, Attitudes And Practices of Pediatric Intensive Care Nurses Related To Using Physical Restraints] Türkiye Çocuk Hast. Derg. Turkish J. Pediatr. Dis. 6(3): 155-160.
|
| [7] |
Regan Judy J, Wilhoite Kerri, Faheen Uzma, Wright Arvis. The use of restraint in psychiatric settings. The Journal mental health series. Tenn Med. 2006Mar: 41-2.
|
| [8] |
Radziewicz RosanneM, Amato Shelly, Bradas Cheryl, Mion Lorraine C. Use of physical restraints with elderly patients. 2009Feb. Available from:
http://www.consultgerirn.org/topics/physical_restraints/
|
| [9] |
Berzlanovich, A. M., Schöpfer, J., & Keil, W. (2012) Deaths due to physical restraint. Dtsch ArzteblInt. 109: 27-32.
|
| [10] |
Hakverdioglu, G., Demir, A., & Ulusoy, F. (2006) Evaluation of emergency nurses’ knowledge on physical restraints. Türkiye Klinikleri J. MedSci. 26, 634-641 (in Turkish).
|
| [11] |
Kalula, S. Z., & Petros, S. G. (2016) Use of physical restraint in hospital patients: A descriptive study in a tertiary hospital in South Africa. Curationis 39(1): 1-8.
https://doi.org/10.4102/curationis.v39i1.1605
|
| [12] |
Lielt Mersha (2019). Assessment of Knowledge, Attitude, Practice And Associated Factors Towards Use Of Physical Restraint Among Nurses Working In Adult Icu In Federally Administered Hospitals Addis Ababa, Ethiopia. Thesis for masters of science degree in emergency medicine and critical care nursing in Addis Ababa.
|
| [13] |
Abeer El-Said, H. E. & Ragaa Gasim, A. M. (2018). Assessment of nurse's knowledge, attitudes, and practice regarding physical restraints among critical ill patients. National Journal of Advanced; 4(1): 15-22.
|
| [14] |
Kaya, H., & Dogu O. (2018). Intensive Care Unit Nurses’ Knowledge, Attitudes And Practices Related To Using Physical Restraints. International Journal of Caring Sciences, 11:1, 61-70.
|
| [15] |
Kandeel N. A. & Attia, A. K.: Physical restraints practice in adult intensive care units in Egypt. Nursing and Health Sciences. 2013; 15, 79–85.
|
| [16] |
Swee, G. L. and Vivian, J. T. (2021). Critical care nurses’ knowledge, attitudes and practices on the usage of physical restrainer. IEJSME; 15 (1): 5-18.
|
| [17] |
Fatma, B. & Fatmana, İ. (2019). The Knowledge, Attitudes and Practices of Nurses in Relation to the Use of Physical Restraints. International Journal of Health Sciences; 7(1): 18-25. URL:
https://doi.org/10.15640/ijhs.v7n1a3
|
| [18] |
Gunawardena, R., & Smithard, D. G. (2019). The attitudes towards the use of restraint and restrictive intervention among health care staff on acute medical and frailty wards- A brief literature review. Geriatrics (Basel), 4(3), 50.
https://doi.org/10.3390/geriatrics4030050
|
| [19] |
Mahmoud AS. Psychiatric Nurses’ Attitude and Practice toward Physical Restraint. Arch. Psychiatr. Nurs. 2017; 31: 2-7.
|
| [20] |
Om-Mohamed Abed El-Latief Nurses’ Knowledge, Attitude and Practice towards Safety Physical Restraint Zagazig Nursing Journal January; 2015 Vol. 11, No. 1.
|
Cite This Article
-
APA Style
Kidane, H., Habtemariam, M., Tewelde, R., Mahmud, S., Habte, E. (2024). Assessment of Knowledge, Attitude and Practice of Nurses’ Towards Physical Restraints for Critical Ill Patients in Orotta National Referral Hospital. World Journal of Medical Case Reports, 5(1), 1-12. https://doi.org/10.11648/j.wjmcr.20240501.11
 Copy
|
Copy
|
 Download
Download
ACS Style
Kidane, H.; Habtemariam, M.; Tewelde, R.; Mahmud, S.; Habte, E. Assessment of Knowledge, Attitude and Practice of Nurses’ Towards Physical Restraints for Critical Ill Patients in Orotta National Referral Hospital. World J. Med. Case Rep. 2024, 5(1), 1-12. doi: 10.11648/j.wjmcr.20240501.11
Copy
|
Download
AMA Style
Kidane H, Habtemariam M, Tewelde R, Mahmud S, Habte E. Assessment of Knowledge, Attitude and Practice of Nurses’ Towards Physical Restraints for Critical Ill Patients in Orotta National Referral Hospital. World J Med Case Rep. 2024;5(1):1-12. doi: 10.11648/j.wjmcr.20240501.11
Copy
|
Download
-
@article{10.11648/j.wjmcr.20240501.11,
author = {Hisabu Kidane and Merhawi Habtemariam and Rahel Tewelde and Sulieman Mahmud and Eyasu Habte},
title = {Assessment of Knowledge, Attitude and Practice of Nurses’ Towards Physical Restraints for Critical Ill Patients in Orotta National Referral Hospital
},
journal = {World Journal of Medical Case Reports},
volume = {5},
number = {1},
pages = {1-12},
doi = {10.11648/j.wjmcr.20240501.11},
url = {https://doi.org/10.11648/j.wjmcr.20240501.11},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.wjmcr.20240501.11},
abstract = {Background: Physical restraint can be defined as any act that avoids a person's liberated body change to a position of preference and, or regular evaluation to their body by the application of any technique, attached or adjacent to a person’s body that they cannot manage or remove easily. Inappropriate use of physical restraints may cause patients grave damage. Different studies informed that patients faced to physical restraints pass on due to pneumonia, constipation, and incontinence, as well as circulatory and respiratory problems. Critical care nurses should make correct decisions regarding use of physical restraints if they are to guarantee patient safety by the accountable nurse. Aim: the intention of this study was to assess nurses’ knowledge, attitude and practice; towards physical restraints use. Method: study design was a descriptive cross Sectional that used to assess knowledge, attitude and practice of nurses towards physical restraints in Orotta national referral hospital with self-administered questionnaire. Lastly data was analyzed using SPSS version 26. Results: the study was conducted among 100 nurses. 60% of the respondents were females and the median age of the study participants was 28 (IQR=6) years, with a minimum age of 21 and maximum age of 50yrs. Most of the study participants 31% had age of 25 or less years. Majority of them were diploma level and did not take any physical restraint related training 55% and 84% respectively. Except in recovery (12%) and adult ICU (27%) areas, the number of nurses in medical, surgical and adult was similar (each 20%). More than ninety percent (94%) of the study participants were not aware of the presence of guidelines regarding physical restraint in their work area. Conclusion: In this current study we concluded that, there was no correlation between knowledge and attitude and also between attitude and practice. But there was correlation between knowledge and practice. Those who have good knowledge can practice well. Nursing implication: By evaluating the current nurses’ knowledge, attitude and practice, this study will contribute recommendation on the frequent training of nurses on physical restraints and possible avoidance of it or safe practice.
},
year = {2024}
}
Copy
|
Download
-
TY - JOUR
T1 - Assessment of Knowledge, Attitude and Practice of Nurses’ Towards Physical Restraints for Critical Ill Patients in Orotta National Referral Hospital
AU - Hisabu Kidane
AU - Merhawi Habtemariam
AU - Rahel Tewelde
AU - Sulieman Mahmud
AU - Eyasu Habte
Y1 - 2024/08/20
PY - 2024
N1 - https://doi.org/10.11648/j.wjmcr.20240501.11
DO - 10.11648/j.wjmcr.20240501.11
T2 - World Journal of Medical Case Reports
JF - World Journal of Medical Case Reports
JO - World Journal of Medical Case Reports
SP - 1
EP - 12
PB - Science Publishing Group
SN - 2994-726X
UR - https://doi.org/10.11648/j.wjmcr.20240501.11
AB - Background: Physical restraint can be defined as any act that avoids a person's liberated body change to a position of preference and, or regular evaluation to their body by the application of any technique, attached or adjacent to a person’s body that they cannot manage or remove easily. Inappropriate use of physical restraints may cause patients grave damage. Different studies informed that patients faced to physical restraints pass on due to pneumonia, constipation, and incontinence, as well as circulatory and respiratory problems. Critical care nurses should make correct decisions regarding use of physical restraints if they are to guarantee patient safety by the accountable nurse. Aim: the intention of this study was to assess nurses’ knowledge, attitude and practice; towards physical restraints use. Method: study design was a descriptive cross Sectional that used to assess knowledge, attitude and practice of nurses towards physical restraints in Orotta national referral hospital with self-administered questionnaire. Lastly data was analyzed using SPSS version 26. Results: the study was conducted among 100 nurses. 60% of the respondents were females and the median age of the study participants was 28 (IQR=6) years, with a minimum age of 21 and maximum age of 50yrs. Most of the study participants 31% had age of 25 or less years. Majority of them were diploma level and did not take any physical restraint related training 55% and 84% respectively. Except in recovery (12%) and adult ICU (27%) areas, the number of nurses in medical, surgical and adult was similar (each 20%). More than ninety percent (94%) of the study participants were not aware of the presence of guidelines regarding physical restraint in their work area. Conclusion: In this current study we concluded that, there was no correlation between knowledge and attitude and also between attitude and practice. But there was correlation between knowledge and practice. Those who have good knowledge can practice well. Nursing implication: By evaluating the current nurses’ knowledge, attitude and practice, this study will contribute recommendation on the frequent training of nurses on physical restraints and possible avoidance of it or safe practice.
VL - 5
IS - 1
ER -
Copy
|
Download